Dressing changes: The outer dressings must be changed regularly to monitor the state of the wound.
Hydrotherapeutic immersion: Hydrotherapeutic immersion of the patient should be avoided as it may prevent proper integration of the NEVELIA® Bi-Layer Matrix or cause early separation of the silicone layer.
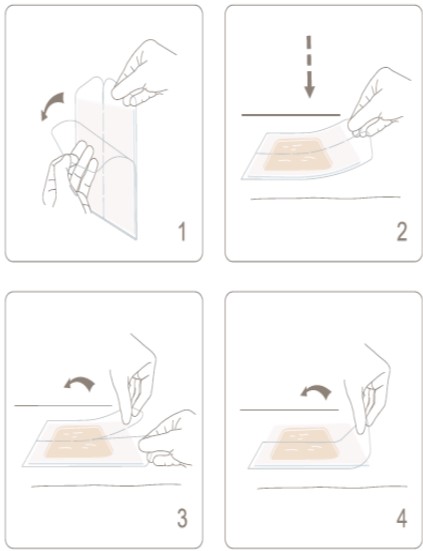
Patient mobility : All inadvertent movement-related disturbance of the NEVELIA® Bi-Layer Matrix should be avoided as this may cause it to separate from the wound bed. Physiotherapy and joint mobility exercises are possible as soon as the patient is well enough, and with the physician’s approval.
Outpatient treatment patients undergoing reconstructive surgery who are discharged home or transferred to another healthcare facility pending the thin split thickness skin graft should be monitored by their attending physician. All the necessary precautions must be taken to protect the NEVELIA® Bi-Layer Matrix from mechanical displacement and/or contamination.